

Abstract
Introduction: Failure rates ranging from 1.7-3.8% of the pegfilgrastim on-body injector (PEG-OBI) device have been reported (Joshi, Curr Med Res Opin 2017; Stuessy, J Clin Onc 2017; Mahler, Clin J Onc Nurs 2017). Failures may increase the risk of chemotherapy-induced febrile neutropenia (FN) and FN-related hospitalizations (FN-HOSP) beyond the FN and FN-HOSP rates for prophylaxis with single-injection pegfilgrastim (PEG) or daily injections of reference (REF-FIL) or Sandoz filgrastim biosimilar (BIOSIM-FIL). We aimed to estimate for a US panel of 10,000 patients with non-Hodgkin lymphoma (NHL) the total incremental costs of PEG-OBI prophylaxis and incremental FN-HOSP costs at different PEG-OBI failure rates versus (vs) assured prophylaxis administration with PEG, REF-FIL, or BIOSIM-FIL.
Methods: Simulation analysis from a US payer perspective of the total incremental prophylaxis costs associated with PEG-OBI failure rates of 1-5% compared to assured prophylaxis administration with PEG, REF-FIL, and BIOSIM-FIL in chemotherapy cycle 1 for a panel of 10,000 NHL patients. Filgrastim daily injection regimens included real-world durations of 5 (Gascón, Support Care Cancer 2016) and 6.5 days (Weycker, Ann Pharmacother 2006) and standard 11 days, all clinician-administered. Differential base rates of FN-HOSP (rate of FN-HOSP without colony-stimulating factor [CSF] minus rate with CSF) in NHL patients was computed for two chemotherapy regimens: 1) cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP) (Chrischilles, Cancer Control 2002; 13.25% with CSF, 23.28% without), and 2) CHOP or cyclophosphamide, mitoxantrone, vincristine and prednisone (CNOP) (Osby, Blood 2003; 33.0% with CSF, 50.0% without). Costs (US$) were based on 1Q2018 average selling price for drugs and 2018 Current Procedural Terminology reimbursement for administration. FN-HOSP costs in 2012 of $25,676 per episode for NHL patients (Tai, J Oncol Pract 2017) were adjusted per the Consumer Price Index for Medical Care to $29,938.63 for 2018.
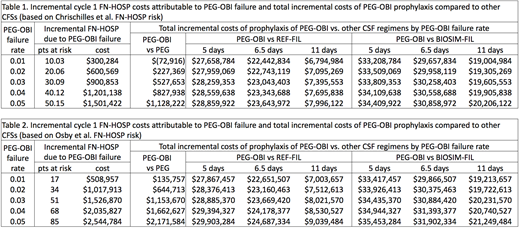
Results: Table 1 (Chrischilles; CHOP) and Table 2 (Osby; CHOP/CNOP) present, for PEG-OBI failures rates of 0.01-0.05, the incremental number of patients at risk for FN-HOSP and associated incremental costs; and total incremental costs of PEG-OBI prophylaxis over the costs of assured prophylaxis administration with other CSFs in CTX cycle 1 for a panel of 10,000 NHL patients. Except for one scenario (savings of $72,916 at 0.1 failure rate due to the lower PEG-OBI administration costs), all scenarios showed incremental costs associated with PEG-OBI prophylaxis and failures of the PEG-OBI device (Tables 1 and 2). Per Chrischilles rates, in a panel of 10,000 NHL patients, incremental FN-HOSP costs due to PEG-OBI device failure ranged from $300,284 (at 0.01 failure rate) to $1,501,422 (at 0.05 failure rate). Total incremental costs of PEG-OBI over PEG ranged from $227,369 to $1,128,222. Total incremental costs of PEG-OBI over REF-FIL ranged from $6,794,984 to $28,859,922; and over BIOSIM-FIL from $19,004,984 to $34,409,922. Per the Osby rates, in a panel of 10,000 NHL patients, incremental FN-HOSP costs due to PEG-OBI device failure ranged from $508,957 to $2,544,784. Total incremental costs of PEG-OBI over PEG ranged from $135,757 to $2,171,584; over REF-FIL from $7,003,657 to $29,903,284; and over BIOSIM-FIL from $19,213,657 to $35,453,284.
Conclusions: In this simulation of NHL patients treated with CHOP or CNOP, the total incremental costs of PEG-OBI prophylaxis vs assured prophylaxis administration with other CSFs vary as a function of PEG-OBI failure rates, baseline and failure-associated FN-HOSP risk, and the alternative CSF prophylaxis option. Incremental costs of PEG-OBI prophylaxis and failure are lowest vs PEG and highest vs BIOSIM-FIL at real-world duration of 5 days.
Krendyukov:Sandoz: Employment. Mathieson:Sandoz: Employment. Campbell:Sandoz Inc.: Employment. Balu:Sandoz Inc.: Employment. MacDonald:Sandoz: Consultancy. Abraham:Sandoz: Consultancy.

